Simon Vassallo,
Performance Audit Manager ,National Audit Office of Malta
Asian Journal of Government Audit

Simon Vassallo,
Performance Audit Manager ,National Audit Office of Malta
Supreme Audit Institutions (SAIs), through their core audit work, play a critical role in promoting transparency, accountability, and improved governance within the public sector. While the more traditional approach to SAI audits focuses on individual entities and/or programmes, contemporary public policy increasingly transcends organisational boundaries, thereby becoming increasingly dependent on coordinated action across multiple ministries, agencies, and service providers. Government efforts in fields such as population ageing, healthcare delivery, climate change and social protection, all involve complex governance arrangements, requiring a whole-of-government approach and policy coherence, that cannot be fully understood through isolated audits.
In view of this, integrated and cross-cutting audits are gaining traction, and their impact is becoming better recognised. Such reviews are taking the evaluation of efficiency, effectiveness and economy to a whole new level, thereby enabling a deeper operationalisation of the fundamental principles of Performance Auditing as laid out in the International Standards of Supreme Audit Institutions (ISSAIs), particularly ISSAI 300 and ISSAI 3000.
However, auditing a single issue across multiple institutional boundaries is likely to present significant methodological challenges. Among others, responsibilities may be fragmented across entities, data systems may be incompatible, documentation retention protocols may diverge significantly from one entity to the next, and policy frameworks may lack clearly defined coordination mechanisms. Addressing these challenges requires careful audit planning, robust analytical frameworks, and extensive engagement with stakeholders.
As an insight to the above, this article explores the Performance Audit: Home-Based Medical and Clinical Services for the Elderly, published by the National Audit Office (NAO) of Malta in December 2025, as a case-study. While this audit was published as a national report, it was carried out as part of EUROSAI’s Parallel Audit on State Preparedness for Population Aging (which is earmarked for publication in 2026).
Malta has been experiencing a clear demographic shift, moving decidedly towards an ageing population. The proportion of older persons within the population has steadily increased over the years, which reflects similar demographic trends observed across developed countries. Longer life expectancy, combined with declining fertility rates, has contributed to a gradual rise in the number of elderly persons within Maltese society.
This demographic shift is evident in Malta’s population pyramid (Figure 1 refers). The base of the pyramid, representing younger age groups, has gradually narrowed due to declining birth rates, while the upper age cohorts have expanded. This transition results in material implications for public service provision, particularly those related to healthcare.
Figure 1: Malta’s Population Pyramid as at end 2024
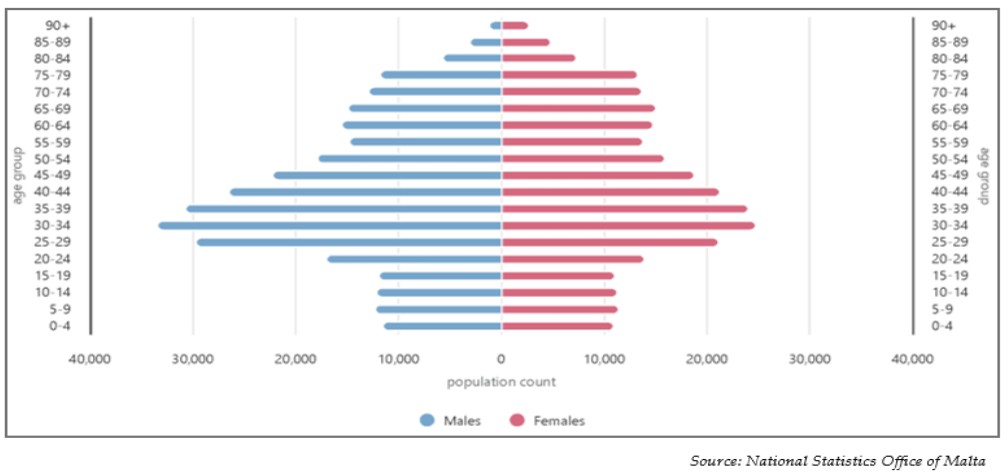
Source: National Statistics Office of Malta
Migration trends have partly mitigated the pace of demographic ageing in Malta. In recent years, inward migration has increased the number of working-age residents, thereby supporting the labour force segment of the Maltese population and somewhat balancing the latter’s overall structure. Notwithstanding, the future inward and outward flow dynamics of this migration are still uncertain, and so are their impacts on the projected composition of the local population and any evolving needs thereof.
By the end of 2024, individuals aged 60 years and over accounted for approximately 23.7% of Malta’s total population, with around 93% of these continuing to reside in their own homes rather than in institutional care settings. This pattern underscores the importance of policies and services that support “ageing in place” and which enable elderly persons to maintain independence within their communities for as long as possible.
Taken together, these demographic developments point to a sustained increase in demand for healthcare, long-term care, and community support services targeted at older persons. To this end, ensuring that adequate systems are in place to support elderly individuals living in the community (including the provision of home-based medical and clinical services), will therefore remain an important policy priority for the foreseeable future.
Malta provides a broad range of home-based medical and clinical services for persons aged 60 and over, delivered through several government entities operating under the remit of the Ministry for Health and Active Ageing.
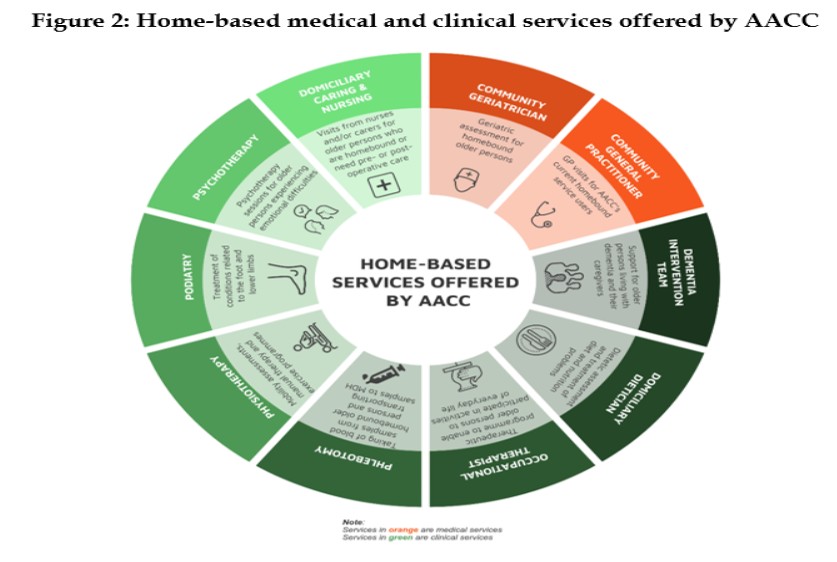
A key role in this system is played by the Department of Active Ageing and Community Care (AACC), which offers a wide portfolio of community-based services primarily focused on non-acute care for older persons (Figure 2 refers). Access to most services requires an application accompanied by a medical report from a general practitioner or consultant. Following submission, the application is assessed by the relevant professional team before services are approved and initiated.
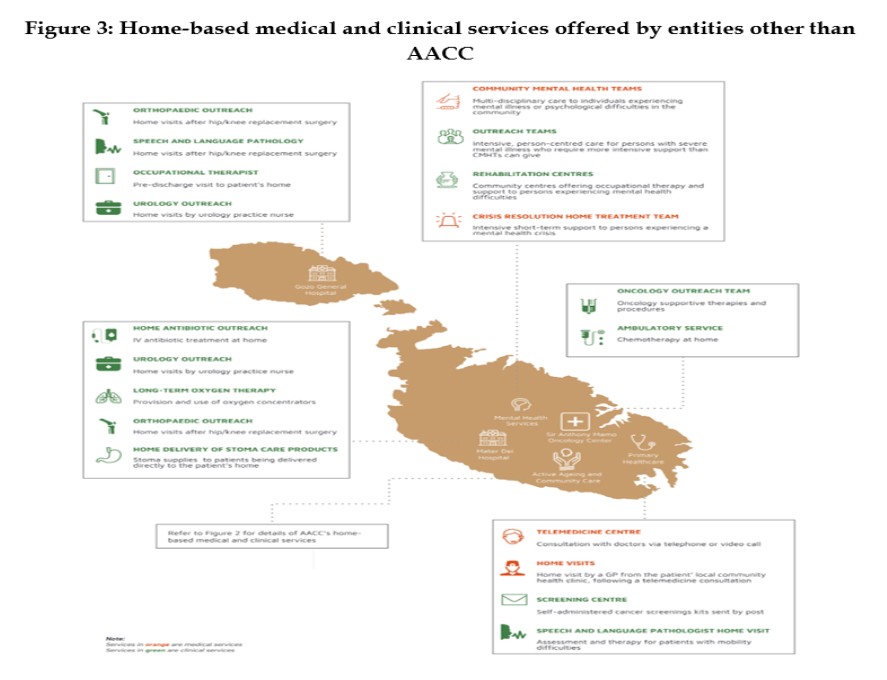
Alongside AACC, several healthcare institutions deliver specialised home-based services where clinically appropriate. The Primary Health Care (PHC) system in Malta is responsible for delivering public primary care services nationwide, primarily through strategically located health centres, but also through a number of home-based services. It also provides cancer screening services, community clinics and telemedicine services.
A number of hospital-based institutions also provide home-based services when clinically required. Mater Dei Hospital (MDH), Malta’s main public hospital, offers certain services delivered in patients’ homes, although eligibility is determined by clinical need rather than age. Where patients discharged from MDH require ongoing community-based assistance, they may be referred to AACC through its standard application procedures.
Within the grounds of MDH, the Sir Anthony Mamo Oncology Centre (SAMOC) provides specialised oncology and haemato-oncology services, including follow-up care that may extend to the patient’s home where appropriate.
Mental well-being within Maltese society is seen to by government through the Mental Health Services (MHS), which provides a comprehensive and integrated range of community and hospital-based mental health services. Specialised multi-disciplinary teams deliver care and support to individuals with mental health conditions who require specialist treatment, while also offering guidance and assistance to their social networks. Access to community-based services requires, in the first instance, a referral from either the patient’s local health centre or by their personal GP, to the community mental health team within the patient’s particular catchment area.
The Gozo General Hospital (GGH) is the only hospital on Malta’s sister island of Gozo, providing acute and complex services, emergency services, inpatient and outpatient services and community outreach services. In addition, the hospital caters for psychiatric and long-term care, and offers home-based follow-up services to its patients based on clinical need.
Figure 3 below maps out these institutions and the home-based medical and clinical services they respectively offer to the Maltese population.
As home-based medical and clinical services for the elderly in Malta are delivered by multiple entities rather than organised under a single department or access channel, the audit team undertook extensive efforts to obtain the information required for this review, involving multiple requests for information and subsequent analysis. For instance, the mapping of all available related services proved to be an onerous task, as a single repository listing all of these could not be found. To this end, while NAO invested significant time and effort to ensure that all services are duly captured in its review, it could not completely exclude that others could potentially exist. Notwithstanding, the audit team still had due comfort that the services captured in this audit constitute the absolute majority of services, and are those of most significance, both in terms of materiality and relevance.
The decentralised nature of the local scoped services resulted into equally decentralised data repositories. This meant that information reaching the audit team was never structured the same way from one entity to another, requiring significant data harmonisation processes. In addition, the manner by which data was kept by most of the scoped entities is largely targeted at providing a national perspective, and proved limited in the possibilities of how this could be filtered to focus on 60+ individuals and/or on services which are provided in a patient’s own private residence (as opposed to, for example, in elderly residential homes). This was arguably the most material limitation for this review, as it considerably constrained the extent and possibilities of analyses. This issue’s impact on this study was significant to an extent that, in a number of instances, the audit team had to re-engineer its analyses to a qualitative approach from its original plan of a quantitative review. This limitation also constrained NAO to make, and declare, a number of assumptions and/or extrapolations when presenting quantitative information in this audit report.
The “Performance Audit: Home-Based Medical and Clinical Services for the Elderly” showed that elderly individuals in Malta are offered a well-developed range of medical and clinical services in their own homes (even if several of which are offered to all age groups within the local population and are not specifically intended for people aged 60+) and that the uptake for these has registered an overall increase during the scoped period. Their provision is however accessed through multiple government entities, which creates challenges when it comes to the elderly managing a collection of such services. While the need for improved collaboration and integration between entities is acknowledged in the National Health Systems Strategy (NHSS) itself, this document does not lay out clearly defined strategic objectives on the further development, enhancement or expansion of these home-based medical and clinical services to the elderly. The same can be said for the National Strategic Policy for Active Ageing, the National Dementia Strategy and Mental Health Strategy.
The challenges encountered by this Office in filtering financial and human resource data to relate specifically to home based medical and clinical services for the elderly (from the information forwarded by the abovementioned audited entities), imply that government is currently not actively seeking to encapsulate and cost these scoped services as an overall distinct concept. This is supported by the observation that the reviewed national strategies only mention these peripherally, as well as by the fact that no readily available trends and/or projections for these services could be found.
With various indicators pointing clearly at the expected increase in the demand for such services, NAO strongly recommended that information management structures are further enhanced so that related financial and operational data (including that relating to staffing levels of medical and clinical professionals) can be easily extracted and comprehensively compiled. These data would prove to be pivotal strategy inputs if the continued provision and further development of these services (possibly through better coordination between the involved entities) is to be considered in the long term, and/or further acknowledged as an independent concept within the national health system.
In the case-study presented above, conducting separate audits on each involved entity would likely have produced insights which are fragmented and limited to individual organisational performance. By contrast, the adopted cross-cutting audit approach enabled the NAO to examine how these entities collectively contribute to a shared policy objective—supporting elderly persons living within the community.
Among others, this system-wide perspective made it possible to identify issues that would have been difficult to detect through isolated audits, such as fragmentation in service delivery, gaps in coordination mechanisms, and limitations in integrated data availability. At the same time, the approach highlighted how different services complement one another within the broader healthcare ecosystem.
Ultimately, this case-study demonstrates that cross-cutting performance audits provide a more holistic and policy-relevant assessment of government interventions, strengthening accountability not only at the level of individual entities but across the entire service delivery system. Such approaches are increasingly important for SAIs as governments rely more heavily on interconnected institutional arrangements to address complex societal challenges.